Submit your Abstracts for the 2025 SSTAR Conference!
We are delighted to invite you to submit an abstract for the 50th SSTAR annual meeting to be held in Philadelphia from April 24 – 27, 2025! The theme of the 2025 conference is Sexuality, Trauma, and Healing. Abstracts on all sexuality-focused empirical research, clinical observations, and theoretical formulations are welcome, and we particularly encourage submissions that focus on trauma’s impact on sexuality. This includes but is not limited to work that examines (a) the role of different types of trauma on sexual outcomes, (b) the mechanisms by which trauma influences sexual well-being, pleasure, functioning, and related outcomes, and (c) processes implicated in recovery and healing.
There are two things that we would like to highlight:
As a new addition to this year's SSTAR Meeting, you have the opportunity to select one of two categories for abstract submissions: (1) Research-focused abstracts or (2) Clinically oriented abstracts. This change allows speakers more flexibility in presenting clinical, empirical, or conceptual content, while SSTAR remains deeply committed to integrating research and clinical work. Additional information is provided below.
All abstracts are to be submitted through Oxford Abstracts, an abstract management software that will makes it easy to organize, review, and standardize all submissions. The submission portal is now open and will remain open until the deadline, October 31, 2024
The following details the information you need to submit an abstract. It is organized in the following sections:
- What needs to be included in a research abstract?
- What needs to be included in a clinical abstract?
- How will abstract be evaluated?
- When will I receive the decision?
- Sample Research Abstract
- Sample Clinical Abstract
- What does the Oxford Abstract submission portal look like?
REASEARCH ABSTRACT SUBMISSION
Abstracts should be no longer than 400 words.
The research abstracts should include the following headings: (a) background/literature review, (b) method, (c) results, (d) discussion, (e) clinical implications of the work, and (f) include 2-3 behavioral learning objectives, and (g) references. The learning objectives state what audience members should be able to do differently as a result of your presentation. The behavioral learning objectives should use action verbs like explain, discuss, compare, define, identify, recognize, use, predict, detect, appraise, diagnose, or interpret, and should avoid vague verbs like appreciate, know, learn, understand, or believe.
CLINICAL ABSTRACT SUBMISSION
Abstracts should be no longer than 400 words.
As this is a new submission category, we provide some examples of types of submissions that could fall under this category. Such examples are illustrative, not exhaustive. Examples include: (1) Identifying a neglected perspective in sex therapy (e.g., a power dynamic analysis of sexual desire discrepancy); (2) Identifying the core features of a disorder that tend to be assessed/diagnosed in variable ways; (3) Providing novel perspectives/insights into disentangling clinical comorbidities; (4) Discussing specific challenges when applying treatment models to minoritized populations; (5) Conceptualizing clinical problems/issues from an intersectional lens; (6) Original work investigating the intersection of sex therapy with historical, political, and socioreligious perspectives; (7) Integrating transtheoretical and transdiagnostic vulnerability factors, such as experiential avoidance and anxiety sensitivity, with assessment and treatment of sexual problems; (8) Describing an integrative approach to the assessment, case conceptualization, or treatment of sexual problems for which limited empirical evidence exists; (9) Critically analyzing some of the mainstream clinical practices in sex therapy and identifying areas for growth/change.
The structure for the clinical abstract should include the following headings.
Background/Objective(s): Identify the key issue(s) you will be investigating in your presentation, highlighting the originality of your questions and/or methods.
Methods: Identify the methods you used in your work. These can include clinical observation, theoretically guided critical analyses, contextual analyses, and/or a critical analysis of assessment or treatment approach.
Conclusions: What are the key takeaway messages of your presentation?
Research Implications: The implications of your work for research will vary depending on the specific topic you are discussing. For some presenters, the implications section may focus on how research is conducted or disseminated. Alternatively, you may want to focus on how future research can help to further clarify some of the questions you raised in your presentation. We encourage presenters to tailor this to their specific content.
All abstracts should include 2-3 behavioral learning objectives that state what audience members should be able to do differently as a result of your presentation. The behavioral learning objectives should use action verbs like explain, discuss, compare, define, identify, recognize, use, predict, detect, appraise, diagnose, or interpret and should avoid vague verbs like appreciate, know, learn, understand, or believe.
Reference section: List some key references related to your work.
HOW WILL ABSTRACTS BE EVALUATED
All abstracts will go through a blinded review process. Abstracts will either be accepted as poster presentations or as oral presentations. There will be two categories of oral presentations: one category will be a 15-minute presentation, and the second category will be a 10-minute data blitz presentation. This decision regarding whether an accepted abstract will be a poster presentation, a15-minute oral presentation, or a data blitz presentation will be based on: (1) judges’ ratings; (2) the extent to which the abstract aligns with the theme of the conference; (3) the extent to which the topic is of broad versus niche interest; (4) the extent to which the work represents innovative and cutting-edge ideas and methods. Abstracts selected for oral presentations will be those that are more aligned with the conference theme, cover topics of broad interest, and represent innovative and cutting-edge work. The decision-making process will also try to ensure that we have a range of topics and methods that relate to different aspects of the conference theme. We will also consider the extent to which the study methods attended to the inclusion of individuals from diverse sexualities and racial identities, if these criteria are relevant within the scope of the presentation.
ABSTRACT DECISIONS
- You will receive a decision on your submission by December 15, 2024.
- If accepted, you will be notified whether you have been accepted for a poster presentation or an oral presentation.
- The first category of oral presentations will be 15 minutes in length with an additional 5 minutes for questions and answers. The data blitz presentations will be ten minutes in length.
SAMPLE - RESEARCH ABSTRACT
Sexual Function in the Nacirema
Since Miner’s initial work on the Nacirema (1956), little further investigation has occurred of this North American group that lives in the territory between the Canadian Cree and the Yaqui and Tarahumare of Mexico. We recently had the opportunity to interview a representative sample of the Nacireman people regarding the prevalence of sexual function difficulties.
Method: Using census data, we randomly sampled 250 Naciremans. We used a translated version of the Universal Survey of Sexual Dysfunction and obtained written informed consent before conducting face-to-face interviews. 87% of the target sample completed the interviews.
Results: Forty percent of the Nacirema reported no problems in their sexual functioning, 30% reported one problem, 20% reported two problems, and 10% reported three or more problems. With regard to problems in the three major areas (desire, arousal, and orgasm), 25% reported a desire problem, 35% reported an arousal problem, and 40% reported an orgasm problem.
Discussion: Comparisons of the prevalence of sexual function concerns in this culture to the prevalence in other cultures are made. The rates of sexual problems in the Nacirema are quite different from those reported in the United States by the National Health and Social Life survey. The levels of complexity and collectivism/individualism in the two cultures do not fully explain these differences.
Clinical Implications: The results of this study will help therapists and researchers working with this population, but are limited by the small sample size.
Behavioral Learning Objectives:
After attending this presentation, the participants will be able to:
- Explain the importance of a representative sample for epidemiological research
- Discuss the prevalence of sexual problems in the Nacirema
- Compare the prevalence of sexual problems in the Nacirema to the prevalence in other cultures
References:
Gingrich, N. & Robertson, P. (1999). On the difficulty of conducting research on sexuality in North America. American Journal of Congressional Impediments, 173, 10-23. doi:XXX7899.GH/8458764
Jagger, M. & Richards, K. (2003). A psychometric evaluation of the Universal Survey of Sexual Dysfunction. International Journal of Psychometrically Adequate Measures, 73, 63-68. doi:XXX7899.GH/8458764
Miner, H. (1956). Body ritual among the Nacirema. American Anthropologist, 58, 504-507. doi:XXX7899.GH/8458764
SAMPLE - CLINICAL ABSTRACT
Conceptualizing Problematic Sexual Desire Discrepancy From Two Theoretical Approaches
Background and Objectives: Sexual desire discrepancies between partners are a common and normative feature of relationships. When desire discrepancies persist or become exacerbated over time, they can become a significant source of distress for one or both partners and are a frequently cited reason for seeking sex/couples therapy. We discuss and compare how two prominent theoretical frameworks, cognitive-behavioral couples therapy and emotion-focused couples therapy, conceptualize sexual desire discrepancies that occur in the context of high relationship distress. We highlight commonalities and distinct features of each conceptualization.
Methods: We conducted a comparative analysis of the two theoretical models, highlighting each theory’s central mechanism of action, points of convergence, and points of divergence.
Conclusions: Both theoretical traditions see the problematic interactions between partners – their ineffective cycles at trying to communicate/solve desire discrepancies – as a factor that contributes to the relationship distress related to the desire discrepancy. However, the two perspectives posit different underlying factors; whereas the couples CBT approach emphasizes the lack of communication skill and the role of negative attributional processes as central to the distress related to desire discrepancy, EFT-based approaches view the negative interactional cycles to be caused by proximal and distal attachment factors, with distal factors representing an individual’s overall relationship with their own and others’ needs and proximal factors being represented by attachment injuries in the current relationship.
Research Implications: Future research needs to test and compare whether the underlying factors posited by each of these theories is supported by empirical evidence. Further, future work needs to integrate principles of sex therapy with these theoretical frameworks to better treat the comorbid sexual issue and the problematic relational dynamics contributing to the sexual problem.
Behavioral Learning Objectives:
After attending this presentation, the participants will be able to:
- Compare the differences between couples CBT and couples EFT conceptualization of sexual desire discrepancies.
- Identify which client features make them better aligned with a CBT versus EFT approach.
- Discuss which mechanisms of actions are central to each theoretical perspective and how they can inform treatment planning.
References:
https://www.bugfreegrains.com/blog/on-grain-treatment/maximize-carryBorden, L., & Allan, R. (2024). Integrating Sex Therapy with Emotionally Focused Therapy to Treat Sexual Desire Discrepancy. The Family Journal, 10664807241264813.
Hoyer, J., Uhmann, S., Rambow, J., & Jacobi, F. (2009). Reduction of sexual dysfunction: by-product of cognitive-behavioural therapy for psychological disorders? Sexual and Relationship Therapy, 24(1), 64-73.
HOW TO USE THE OXFORD ABSTRACT SUBMISSION PORTAL
Below is a step-by-step guide with screenshots to show you the different steps in submitting your abstract using the online portal.
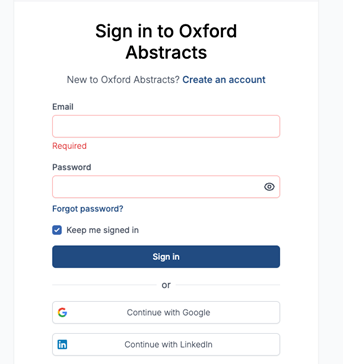
Step 1: Signing into the system. If you have used Oxford Abstracts to submit to another conference, you can use your login information from the previous submission. If you have not used it previously, you will have to create an account.
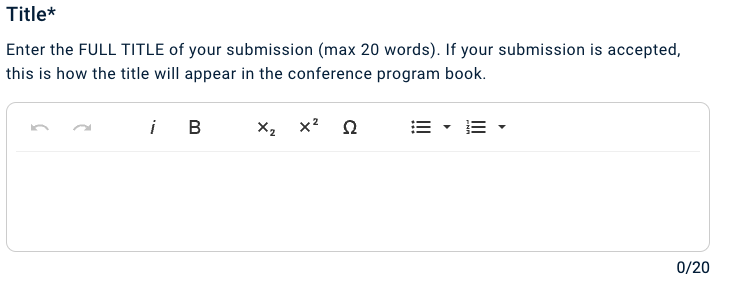
Step 2: Enter the title of your submission. The word limit for the title is 20 words.
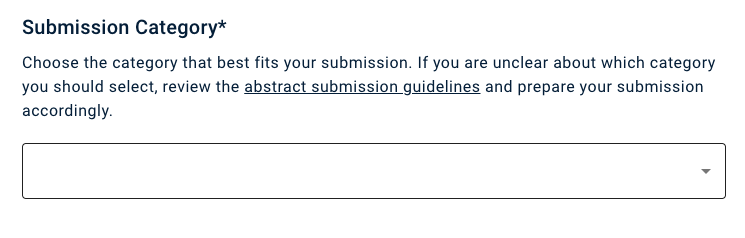
Step 3: If you are submitting a research abstract, select this option from the drop-down menu. If you are submitting a clinical abstract, select this option from the drop-down menu.
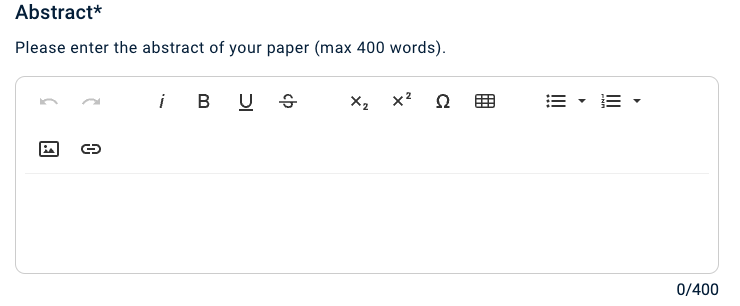
Step 4: Copy and paste your abstract. The word limit for the abstract is 400 words.
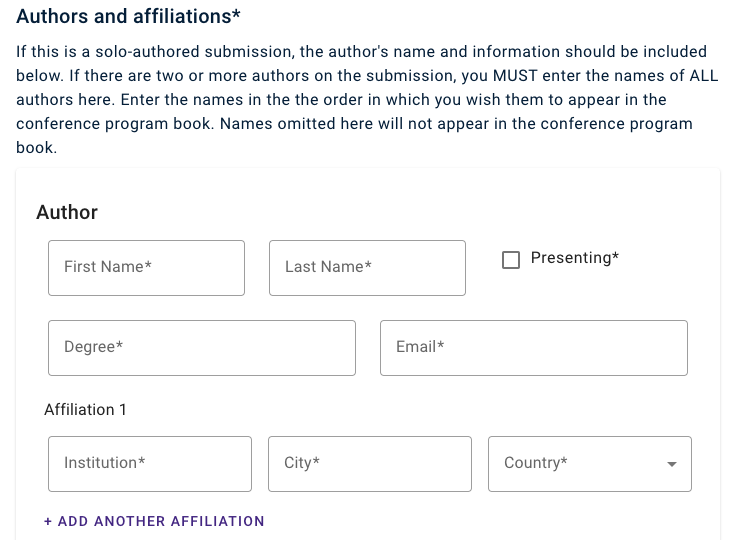
Step 6: List the pronouns for the solo/lead author
Step 7: Upload the CV for the solo/lead author
Step 8: Select whether you are a full-time student or not.
Step 9: Select your current membership status (at the time of abstract submission).
Step 10: Indicate how many SSTAR meetings you have attended by selecting the appropriate category.
Step 9: Complete the following attestations
Final comment: Once you have successfully submitted your abstract, you will receive an email notification that it has been received.